I. Introduction
According to the World Health Organization (2023), around 2.3 billion people globally still rely on polluting fuels for cooking including inefficient stoves, coal and biomass. Consequently, indoor air pollution has led to increased death rates among those living in the same family, particularly women and children. The World Health Organisation reported that there were approximately 3.2 million fatalities in 2020 because of using polluted fuels, of which 237,000 were children under the age of five. Moreover, a substantial body of empirical research has emphasised the health hazards linked to the use of contaminated cooking fuel (Li et al., 2023; Ma & Zheng, 2021; Mpuure, 2023; Raifu et al., 2023; Ren et al., 2022). For instance, Mpuure’s (2023) research in Ethiopia demonstrated that the use of inefficient cooking fuels contributes to indoor pollution, thereby reducing women’s productivity and exacerbating their poverty rates. In terms of health outcomes, research demonstrates that the use of clean cooking fuel leads to long-term health improvement, but it does not show short-term health benefits, which contradicts the notion that women who use clean cooking fuels experience short-term health improvement. Ma et al. (2021) found that rural populations in China experience enhanced personal well-being and overall life contentment when they transition from unclean to clean cooking fuels. Nevertheless, partial transitions do not significantly affect the subjective well-being of households. Luo et al. (2023) found that pregnant women who use polluting cooking fuels face a likelihood of experiencing low birth weight (LBW), stillbirth (SB), and preterm birth (PTB). Byaro et al. (2024) revealed that access to clean fuel significantly reduces maternal, infant, and child mortality rates in Africa.
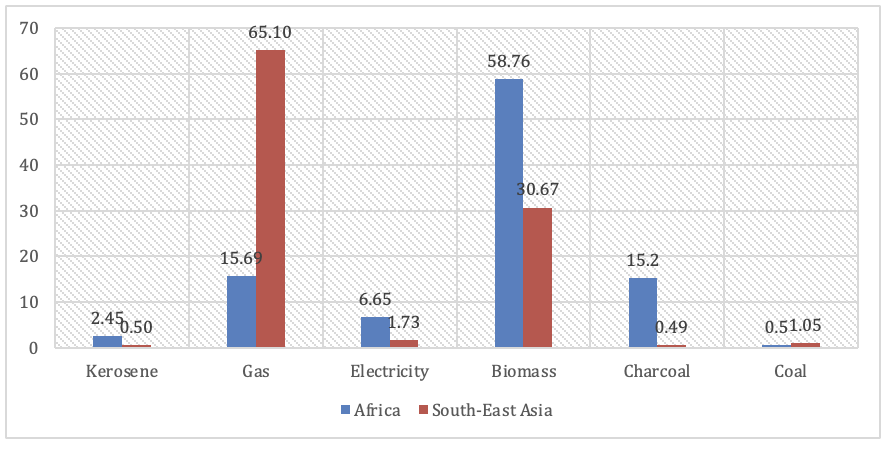
Given the importance of transitioning from dirty to clean cooking fuels, global leaders have included the promotion of clean cooking fuels in the Sustainable Development Goals (SDGs). SDG 7 prioritises the attainment of affordable and clean energy. In pursuit of this goal, several developing countries have made significant efforts to transition from polluting cooking fuels to cleaner alternatives, with significant progress. However, the progress differs by region. For example, while African countries have made some progress, it is relatively small compared to Asian countries. Specifically, the fraction of Africa’s population that relies largely on clean cooking fuels increased modestly from 11.91% in 1990 to 20.31% in 2020. In contrast, in Southeast Asia, this proportion has increased significantly from 10.40% in 1990 to 64.20% in 2020, suggesting tremendous regional progress. Figure 1 in the appendix shows that in 2021 most African countries continue to rely heavily on biomass fuels for cooking, with about 60% of the population doing so. In contrast, gas has become the primary cooking fuel in most Southeast Asian countries, with more than 60% of the population using it for cooking. This significant gap in the transition to clean cooking fuels will undoubtedly have different health outcomes in the two regions.
Given these facts, this study aims to examine how access to clean fuel and technology (ACFT hereafter) affects health outcomes through a comparative analysis of Africa and Asia. The hypothesis is that improvements in ACFT in these two regions have no significant effect on health outcomes. Our research builds on the work of Byaro et al. (2024), who investigated the impact of access to electricity and clean fuels on health outcomes. However, our study differs in some ways. First, we consider a variety of health outcomes, including infant and child mortality, female adult mortality, and life expectancy. We focus on infant and child mortality because children are more susceptible to indoor pollution from dirty cooking fuels than adults, who may have a higher immunity. Additionally, we include life expectancy to determine whether ACFT not only improves overall health but also contributes to longer lifespans. Second, our study extends beyond Africa to include Asia, enabling a comparative analysis of how ACFT impacts health outcomes in the two regions. This comparative approach is crucial for understanding of variations in regional factors such as socioeconomic status and cultural traditions influencing access to clean energy technology. The outcomes of our study could provide a foundation for policy interventions aimed at improving health outcomes across different regions.
Section II presents the methodology and data sources. Section III presents the results while section IV concludes with the policy implications.
II. Methodology and Data Sources
This study uses the Generalised Least Squares (GLS) approach, an estimation method developed by various authors, including Bai, Choi, and Liao (2021). The superior performance of GLS in handling heteroscedasticity, serial and cross-sectional correlations makes it preferred over Pooled Ordinary Least Squares (OLS). The OLS approach may not provide the most unbiased estimates under conditions of heteroscedasticity and correlation. In contrast, GLS demonstrates greater efficiency in such scenarios (Bai et al., 2021).
As a result, we specified a linear panel model to investigate the relationship between access to clean fuel and technology and health outcomes, while also accounting for relevant control variables.
HOit=α0+α1ACFTit+γ′X+εit
where represents health outcomes. When choosing the health outcome factors, we relied on prior research, including the study conducted by Byaro et al. (2024). The variables we chose include infant mortality rate, child mortality rate (under-5), female adult mortality rate, and life expectancy at birth. The variable ACFT denotes access to clean fuel and technology expressed as a percentage of the population. Additionally, we include other variables which are theoretically linked to health outcomes. These variables include GDP per capita, current health expenditure per capita, and population growth. We expect that GDP per capita and health expenditure will have positive or negative effects on health outcomes, depending on the specific measures of health outcomes. The impact of population growth could similarly be positive or negative, depending on the measures of health outcomes.
Depending on data availability, we use panels of 20 countries in each region, spanning the period from 2000 to 2021.[1] We source all variables from the World Development Indicators (WDI).
III. Empirical Findings
We conducted several preliminary tests, including descriptive statistics, a unit root test using the Maddala and Wu method and Pesaran’s cross-sectional dependence test. However, due to word count limitations, we only briefly present the results of the descriptive statistics and unit root test. Table 1 presents the descriptive statistics. The evidence from the table indicates that average infant mortality (IM), child mortality (CM), and female adult mortality (FAM) are significantly higher in Africa (IM-52.75%, CM-80.39%, and FAM-294.93%) compared to Asia (IM-23.56%, CM-29.06%, and FAM-113.8%). Conversely, the average life expectancy is higher in Asia (72.15 years) compared to Africa (59.49 years). Furthermore, the average ACFT is higher in Asia (69.46%) than Africa (38.22%) indicating significant progress in clean energy access on the Asian continent.
Table 2 shows the results of the unit root test. The findings suggest that variables such as child mortality, infant mortality, and access to clean energy and technology are I(0) variables for both Africa and Asia, meaning they are stationary at the level. Conversely, GDP per capita, health expenditure, and population growth are I(1) variables, suggesting they become stationary after the first difference. The life expectancy and female adult mortality variables are I(1) for Asia but I(0) for Africa. Overall, the unit root test results reveal a mixed order of integration.
Table 3 presents the main results that show the impact of ACFT on health outcomes. The evidence from the table generally shows that ACFT improves health outcomes in both Asia and Africa, with varying degrees of impact. Specifically, ACFT reduces infant mortality, child mortality and female adult mortality and improves life expectancy. Thus, an increase in ACFT by 1% will reduce infant mortality, child mortality, and female adult mortality by 0.21%, 0.30%, and 0.12% in Asia and 0.21%, 0.27%, and 0.09% in Africa, respectively. Our results corroborate the finding by Byaro et al. (2024) who established the negative effects of ACFT on similar health outcome variables. Furthermore, if ACFT increases by 1%, life expectancy in Asia and Africa will rise by 0.03% and 0.05%, respectively. Generally, our findings show that ACFT improves the health outcomes in both Asia and Africa.
In all models, control variables such as health expenditure and GDP per capita follow a priori expectations, whereas population growth yields mixed results across the models. Expectedly, GDP per capita and health expenditure reduce IF, CM, and FAM and improve LE.
IV. Conclusion and Policy Recommendations
In this study, we have tested the null hypothesis that progress made in Africa and Asia in terms of ACFT does not improve health outcomes. We tested this null hypothesis using data from 20 countries in Africa and Asia, covering the period from 2000 to 2021. To address some panel data method problems, such as heteroscedasticity and serial and cross-sectional correlations, we employed the GLS estimation method.
Our findings show that ACFT indeed improves health outcomes in both Asia and Africa, with varying degrees of impact. This shows that even though there is variation in ACFT in both regions, ACFF is indispensable for improving health outcomes in Asia and Africa. The effect of control variables also follows a priori expectations, as both health expenditure and GDP per capita reduce IF, CM, and FAM, while improving LE. However, population growth produces mixed results.
Based on our findings, we recommend Asian and African governments to prioritise the implementation of policies that enhance access to clean fuel and technology, given their proven ability to improve health outcomes. This includes allocating resources to the development of renewable energy infrastructure and the implementation of efficient cooking technology.
